


Abortions and Cesareans
Originally written by Karl, published in Portuguese at Ecce Medicus.
======================================

Cesareans delivery
– You popped?! How nice! Was it natural?
– Natural, yeah…. For the doctor, right?
Dialogue between a postpartum woman and the author of this article.
It made last week’s headlines the information from the Health Department showing that for the first time, Brazil reported more cesareans than vaginal births in a year: 52% overall. According to an article in Folha de S. Paulo, rate of cesareans in the private sector has been stable since 2004 and is around 80%. In the Public Health System (SUS in Portuguese), that number is increasing and went from 24% to 37% in the last decade.
The term cesarean section does not seem to have anything to do with Julius Caesar, supposedly born of this procedure, as I was taught in college. As Professor Joffre [in Portuguese] emphasizes; “the word cesarean and the expressions cesarean section and cesarean delivery are linked to the Latin verb caedo, caesum, caedere, which is equivalent to the Greek témno, to cut.
From it, derive caesus/a/um, “that which has been cut”; caeso/onis, to slipt or separate; caesura, a cut or cuts; and caesar/aris, the same as decaeso/onis, i.e., one that is taken from the mother’s womb, or “qui caeso matris utero nascitur”.
It is a known fact that Brazil is the world champion in caesareans, and it has been roundly criticized for it (a small collection of links: unnecesarean, guttmacher with a Brazilian reference, another reference in PDF, another Lancet study [subscribers-only], among many others). But as the post title suggests, I would like to make a parallel between abortions and cesarean sections.
Let me first disclaim my conflict of interests; I do not believe in abortion as a contraceptive method in public health because it does not work well as one. But, regardless of what sectors of the Church, the Brazilian Theocratic State, sociologists, doctors, etc want, it is a woman’s prerogative. Abortions should be “accessible, safe and extremely rare,” as it has been said. It is one of the symbols of the gap between Brazilian social classes the way its practice permeates the various segments of the female population of the country: from knitting needles, outlawed abortive pills and pray-for-the-best, to highly-equipped clinics with all the comfort and care of large hospitals. (I won’t even discuss the issues of malformed fetuses and the mother’s risk of death, because it would be too much for this post. See my views on the subject [in Portuguese] here, here and here).
Back to cesareans and the bewilderment caused by it. The cesarean delivery follows the same reasoning as with abortions: it is a woman’s prerogative if she wants to have her baby vaginally or surgically. The problem is that this decision is never fully explained and here enters the role of the physician. I did five natural deliveries during my medical training. In some, I spent the whole night with girls writhing in pain without any relief. If there was no alternative, fine, the gift of motherhood will always compensate for anything, at least that’s what they say. But if there is a different approach in which the risk/benefit ratio is acceptable, why not try it out? Who decides? The MD and the mother, and no one else.
The doctor, however, should play the same as when is presented with someone wanting to have removed an unwanted fetus. Expose, with the highest possible moral exemption, the risks of the procedures and take a position. These are not decisions that are up to patient alone. Saying that one does not do nor prescribe abortive procedures is completely legitimate. The patient should know that this is against Brazilian law and that the doctor who does it is in risk of being sued. With C-sections, the situation is more bland, but similar. There is no law against it, but there are clinical indications more or less needed. If a pregnant woman wants a cesarean section, the physician should explain the risks and take a stand. The problem is that there is a doctor’s bias favoring the procedure. Now we’re putting the fox in the hen house. And with that, I can not agree.
Let’s put some data in this discussion. Obstetricians and the World Health Organization estimates that approximately 15% of deliveries should be cesarean due to complications related to them. If private hospitals in São Paulo City, the rate is around 80%, according to the Folha, there is an excess of 65% in favor of cesarean sections that needs explaining. There is a group called Caesarean Delivery on Maternal Request (CDMR). There are strong indications, according to the Lancet study cited above, that this “movement” has begun in Brazil and spread to other nations. It is estimated that this type of “indication” may account for up to 20% of cases of surgical deliveries. Zhang’s study (below) checked 1.1 millions of non-twin births over 13 years in southeastern China and showed a significant increase in the number of caesarean sections in large part due to CDMR. In some places, the indications at the request of mothers reached 50% of C-sections. In Brazil, Osis and colleagues (below) set out to try to understand why so many cesareans. They studied 656 women in São Paulo and Pernambuco, users of public health services, and divided them into two groups. The first consisted of women who had previously experienced vaginal delivery and then had a cesarean. The other, consisting of women that had gone through only cesarean deliveries. 90.4% of women who had at least one vaginal delivery considered it best, against 75.9% among those who had only cesarean sections (the number of those who had only vaginal deliveries in the study was too small which constitutes an important bias). If those who had cesareans entered into labor, the result would have been similar (45.5% and 42.8%). 47.1% of those who had vaginal delivery said it had no downsides, compared to 30.3% of those who did not. On the other hand, 56.7% of women who only had cesareans reported that having no contractions was the main advantage of the method against 41.7% of the others. The conclusion of the article is that the pain is important, but women classify it as secondary. First comes the child’s health and the recovery from the operation. In addition, in Brazil is very important to be able to perform a tubal ligation (“tying the tubes”) for sterilization and this weighed in choosing the route for delivery. This constitutes a serious flaw of public health policies of those two states with regard to birth control, according to another article. We can not replace one mistake for another.
To conclude this long blog post, I’d say:
1. It is legitimate for a mother to want a cesarean (CDMR), as much as it is legitimate for a mother to not want to carry out an unwanted pregnancy – her prerogatives, exclusively – since she is fully informed of the consequences that such procedures actually involve. (Some people argue about what is “fully informed” saying it is impossible for a layperson to be clarified about procedures with such complex consequences, which creates implications for the informed consent, the instrument without which NO clinical research is done, just so we get a glimpse of the size of the problem we are dealing with).
2. Physicians have a key role in the choice of the delivery route and must rid themselves of their individual preferences to advise the pregnant woman. Given the enormous difficulty in doing this (since a physician trusts their skills for both procedures) is not totally unreasonable to seek a second opinion on the subject. This reduces, without a doubt, any bias. But increases insecurity, another difficult choice.
3. The excess cesareans is an example of the medicalization of Medicine. Like baldness, shyness and restless children [in Portuguese], it shows us how to turn arbitrary “deviations” of normality into technically manageable pathologies.
Photo taken from the blog Parir é Nascer.
![]() Zhang, J., Liu, Y., Meikle, S., Zheng, J., Sun, W., & Li, Z. (2008). Cesarean Delivery on Maternal Request in Southeast China Obstetrics & Gynecology, 111 (5), 1077-1082 DOI: 10.1097/AOG.0b013e31816e349e
Zhang, J., Liu, Y., Meikle, S., Zheng, J., Sun, W., & Li, Z. (2008). Cesarean Delivery on Maternal Request in Southeast China Obstetrics & Gynecology, 111 (5), 1077-1082 DOI: 10.1097/AOG.0b013e31816e349e
![]() Osis MJ, Pádua KS, Duarte GA, Souza TR, & Faúndes A (2001). The opinion of Brazilian women regarding vaginal labor and cesarean section. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics, 75 Suppl 1 PMID: 11742644
Osis MJ, Pádua KS, Duarte GA, Souza TR, & Faúndes A (2001). The opinion of Brazilian women regarding vaginal labor and cesarean section. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics, 75 Suppl 1 PMID: 11742644
Broken heart syndrome and the flagellated heart
This is another one of those unlikely situations that insist on existing. Could a very strong emotion cause a cardiac alteration so severe capable of causing someone’s death?
I’m not talking about arrhythmia. Electric alterations in the heart could make it lose its regular rhythm and, possibly, create a situation where there is, in fact, a cardiac arrest. Arrhythmias may be caused by a number of factors, including electrolytic disorders, traumas, drugs, as well as emotions.
What I am talking about are anatomical alterations, detectable by examination, like echocardiogram or ventriculography done during catheterization. Is it possible for a strong emotion to cause a heart failure?
Yes, it is possible. And this clinical situation is called cardiomyopathy of takotsubo, also known as transient apical ballooning syndrome, apical ballooning cardiomyopathy, stress-induced cardiomyopathy, broken-hearted syndrome or simply stress cardiomyopathy. Takotsubo is a cage for catching octopus in Japan. Due to its balloon-like shape, it was compared to the shape of the heart of someone who suffered a very strong emotion and got seriously compromised (see pictures below).
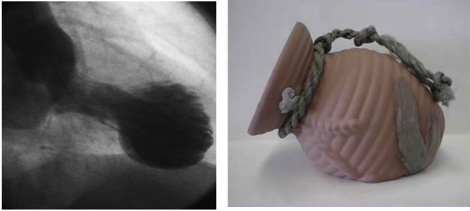
Left. Ventriculography showing large anterior dilation of the heart. Right. Takotsubo jar.
Cardiomyopathy means, literally, “heart muscle disease”. In this case, always a kind of weakness. Because with this disease the weakening follows a strong emotional reaction -loss of children or spouse, for example- it was named “broken heart syndrome”. It is a known cause of lethal arrhythmias and even ventricular rupture, such is the thinning of its wall. The good news is that, after the acute, more dangerous phase, the recovery is complete (ad integrum) without sequellae.
Recently, an article drew attention to the fact that these patients may present themselves in a state of cardiogenic shock that prevent organs from functioning properly because of inadequate blood flow and arterial pressure, such is the heart failure, requiring intensive care resources. In the article, the authors show clinical, laboratorial and echocardiographic differences in patients.
Reading the article I had a brilliant idea!
I could not help remembering my pathology classes where I saw several hearts infected with Chagas disease, a true Brazilian plague.
Many of those hearts present what pathologists call “aneurisma de ponta” (tip aneurysm) (see image on the left, from the excellent article by Eduardo Nogueira from UNICAMP).
This aneurysm of the left ventricular apex is very similar to that produced by the dilation of takotsubo cardiomyopathy.
According to the late professor Köberle, from USP – Ribeirão Preto, the explanation for the tip aneurysm in Chagas disease is an imbalance between the sympathetic and the parasympathetic autonomic nervous systems. Parasympathetic nerve endings disappear from myocardial tissue and there is a sympathetic hyperactivity, “sufficient enough to cause myocardial lesions”. Köberle managed to reproduce the same kind of injury in mice by injecting adrenaline, the hormone of the sympathetic system.
My brilliant idea was to imagine that the explanation for the takotsubo cardiomyopathy was the same! Strong emotions cause an overload of sympathetic stimulation on the heart and could -why not?- cause an anatomic alteration similar to the tip aneurysm of Chagas cardiomyopathy.
I was feeling pretty smart and thought of sending an article to an international cientific journal.
But, as with almost all of my brilliant ideas, someone else got there first.
And, to keep my readers from posting that reference before I do, here it is (also down there at the bottom).
Medal I shall not receive for deserve I do not.
Was gonna write a paper, wrote a blog post instead. Meno male.
Images:
Ventriculography: Nature Medicine; Takotsubo jar: Canadian Journal General Internal Medicine.
Wittstein IS, Thiemann DR, Lima JA, Baughman KL, Schulman SP, Gerstenblith G, Wu KC, Rade JJ, Bivalacqua TJ, & Champion HC (2005). Neurohumoral features of myocardial stunning due to sudden emotional stress. The New England journal of medicine, 352 (6), 539-48 PMID: 15703419
======================================
Originally written by Karl, published in portuguese at Ecce Medicus
When swine flu gets serious
In 2009 the swine flu, caused by the H1N1 virus, was recognized as this century’s first pandemy. In Brazil at least 19,000 people suffered the fever and aches caused by the flu, and over 1,300 were killed.
As it is now the northern hemisphere’s turn to fight the flu, it may be useful to draw from what was learned by researchers from southern countries. Some of it is summarized by Ricardo Zorzetto in the article published in the December issue of Pesquisa Fapesp, a Brazilian science news magazine: in some cases, the immune response against the virus is so strong that it destroys the lungs.
A companion article in the same issue discusses the benefits of vaccination against swine flu in the northern hemisphere. Bellow is a translated version of both stories.
by Maria Guimaraes
==========================================
Exaggerated reaction
Influenza A, H1N1 virus, the cause of swine flu, induces inflammation that destroys lung cells
by Ricardo Zorzetto
In mid-spring, the 2009 flu season came to an end in Brazil. This year, the chief villain was the influenza A, H1N1 virus, the cause of swine flu and of this century’s first pandemic. In the second week of October, the Health Ministry recorded only 78 severe cases of swine flu in Brazil, a dramatic drop (97%) in relation to the mid-August peak. In six months, the H1N1 virus caused at least 19 thousand Brazilians to get a high temperature, along with severe muscular pain and a painful shortness of breath, and killed 1,368 – almost one third of the 4,735 deaths by flu recorded worldwide during this period, when 399 thousand cases were confirmed. As Brazil and other countries started to prepare for the second wave of swine flu that is already spreading in the Northern Hemisphere, as winter approaches, researchers from the University of São Paulo (USP) concluded the first analyses of H1N1 damage to the body. The São Paulo group found that, in the most severe cases, the body produces such a strong immunological reaction that it kills the virus, while also damaging the lungs so heavily that they stop working.
The most obvious sign of such damage is labored breathing (dyspnea), very frequent among those who developed the most serious and sometimes lethal form of swine flu. “All doctors should be alerted to this symptom, which indicates that the infection may be severe,” states pathologist Thais Mauad, from USP, the main author of the study published online on October 29 in the American Journal of Respiratory and Critical Care Medicine, the first to describe systematically the fatal lesions induced by H1N1.
Thais and another 14 researchers from the USP Medical School, who worked under the coordination of pathologists Paulo Hilário Saldiva and Marisa Dolhnikoff, came to this conclusion upon examining samples of different organs of 21 swine flu victims who died in São Paulo. “These cases are representative of the Southeast and South, which accounted for the majority of cases in the country,” states epidemiologist Denise Schout, from the USP team.
Heavy damage – In almost all cases – 20 out of the 21, to be precise – the lungs suffered mass destruction of their alveoli, microscopic cavities within which gas exchanges occur. Though with lower incidence (29% of the people), there was also severe inflammation and cell death in the bronchioles, the ramifications of the tubes that carry the air from the trachea to the lungs. Additionally, in 24% of these cases, bleeding (hemorrhage) due to the bursting of the blood vessels that irrigate the alveoli was also identified.
“This kind of damage is similar to what was observed in other flu pandemics, such as those in 1918, 1957 and 1968, though in the previous ones and in the first one in particular the death rate was far higher,” comments Thais. Another finding that struck the researchers was that 38% of these patients also had infections by Streptococcus pneumoniae, bacteria that cause respiratory system problems. “In cases such as these, it is important to add antibiotics to the antiviral drug treatment,” says Thais. “This information helps us to understand how the infection sets in and advances and, in the future, it can provide guidance for treatment,” comments Denise.
Natural killers – The concentration of the damage in the lungs does not mean that H1N1 only affects these organs. In almost all cases, the virus invades the cells that internally line the upper respiratory tracts (nose and throat), just causing typical flu symptoms: coughing, pain and a runny nose. Only in a very small number of people does the H1N1 escape the layer of mucus that helps to protect the upper respiratory system and reaches the lungs, which are normally sterile, complicating matters – in 7% of such cases, according to data from the USP team, the lung infection becomes so severe that it leads to death.
Microscopic and biochemical analysis of the lungs, however, indicated that the damage to these organs is not caused by the virus directly. Once infected by H1N1, which takes over control of the genetic apparatus, the alveoli cells start to make a chemical signaler, interferon-gamma, which inhibits the multiplication of the virus and activates the defense cells known as natural killers (NK). The NK, in turn, pour toxic compounds into the infected cells inducing the cells’ programmed death, i.e., apoptosis. At a suitable level, this sequence of actions in the defense system eliminates the infectious agents and helps to reestablish the organ’s health. However, when the level is exaggerated, it damages the organ – irreversibly, in some cases.
In the lungs of the fatal victims of swine flu, Thais and Ludhmila Hajjar found interferon-gamma levels and NK cells in numbers far greater than exist in healthy individuals’ lungs. It is not yet known what triggered the exaggerated response. “Some factor that we haven’t identified yet must have created this imbalance,” says Thais. Out of the 21 people analyzed by the USP team, 16 had already suffered from other serious diseases, such as cardiovascular conditions or cancer, before they caught swine flu. In Thais’s opinion, it is likely that their immunity had already been jeopardized, to the point of allowing the infection’s severity to rise sharply. Until answers to these questions are found, experts worldwide believe that the best protection against the virus is to take the vaccine, which some countries have already started distributing.
The second wave and the vaccine
Countries in the Northern Hemisphere start pre-winter vaccination drive
Weeks ago, the United States and China started vaccination drives against the influenza A, H1N1 virus, of swine origin, that caused the flu pandemic in the first half of 2009 and created panic in many countries. Health authorities worldwide consider immunization the chief means of preventing swine flu deaths and of containing the spread of this virus, which started in the Northern Hemisphere even before the onset of winter and is likely to become the chief cause of flu in upcoming years.
Despite the confidence of health administrators in immunization, in countries such as the United States, part of the population is skeptical about having the vaccine. The same feeling that the virus awakened at the beginning of the year is what underlies this doubt: fear. If before people feared the virus’s aggressiveness, now they question the vaccine’s safety and fear its side effects. This is so because, even before trials for safety and effectiveness had been completed, the FDA (the United States Food and Health Administration) released the production and application of two types of H1N1 vaccines: one in injectable form, made from inactive viruses and suitable for any person aged 1 or above; and another in breathable form, made from attenuated viruses and recommended for healthy people aged 2 to 59. As these only protect against swine flu, they are being applied along with the seasonal flu vaccine.
Danielle Ofri, a professor at the New York University Medical School, published an article in November in the New England Journal of Medicine describing the contradictory behavior of people seen at the Bellevue hospital, the oldest one in the United States. At the onset of the epidemic, fear of this unknown virus drove them to demand a vaccine that did not exist. However, now that it is available, most people, being less anxious and more used to the virus, refuse to take it.
Experts have no doubt that the vaccine works, although some disagree as to the level of protection it provides. “Even if the vaccine doesn’t protect 100% of the people, it should protect at least some 75%,” states Edison Durigon, head of the Virology Laboratory at the Biomedical Sciences Institute of the University of São Paulo. According to him, those who have the vaccine may even catch the flu, but it will be less severe. “The vaccine will only lose its effectiveness if the epidemic’s predominant virus variety undergoes very drastic genetic changes, which is rare.” Should this occur, the loss of efficacy will become known in a while, after more people have been vaccinated and the level of protection provided by the vaccine is analyzed.
Up to mid-November, the World Health Organization (WHO) estimated that 65 million people in 16 countries had already taken the H1N1 vaccine. In one report, the WHO stated that in China 11 million people were vaccinated, with 15 cases of serious side effects being recorded and two deaths, although the latter did not necessarily result from the immunization. As the vaccine production will be insufficient for all (WHO expects world production to reach 3 billion doses a year), the priority is to immunize those who are at particular risk: children from the age of one, people with serious diseases and healthcare professionals. In Brazil, where the H1N1 death rate was 0.8 per group of 100 thousand people (the rate of seasonal flu is 0.5 per 100 thousand), the swine flu vaccine is expected to be available before the winter of 2010.
The subsidiary patient
Many times, in my practice, I am required to explain some statistical concepts to my patients in order to make them avoid some frequent pitfalls. The most common concept I explain is what is “normal” in lab exams.
Let’s suppose someone invents a new lab test to measure the glucose in the blood. How would we determine what are the normal values for this test? Once we are certain that the exam will not harm anyone, the researcher start looking for HEALTHY (this is important) subjetcs in order to measure their blood glucose levels. The researcher will probably measure thousands of blood samples, put them in a graph and what will she/he find?
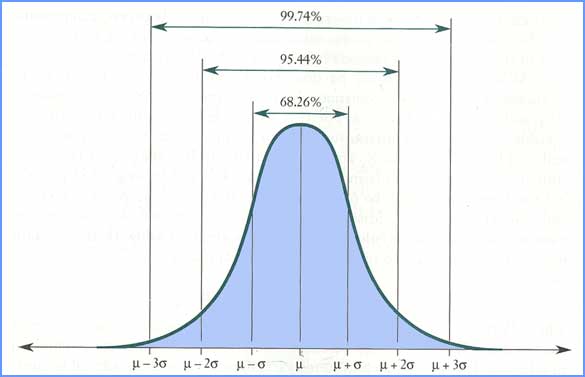
Normal distribution
The normal distribution has some interesting properties. The one we are using in this example is the one above. It is possible to calculate the proportion of the subjects (area under the curve) in each point. If we evaluate the area between μ-2σ and μ+2σ, we will find out that it corresponds to about 95,44% of the whole population Here you are. I thereby declare that the “normal” values in this alb tests are found between μ-2σ and μ+2σ, as 95% of all the healthy people are found in this interval.
Whenever a patient comes to see me, and I decide to test her/his glycemia using the method we have just described, there will be a chance, intrinsic to the method, that it will give a result that is out of the boundaries determined as “normal” limits, even though the patient is completely healthy. This chance, as explained, is about 5% (2.5% for each side of the distribution). Somebody may say: “OK, Karl, nothing is perfect and there is always margin for error.” I agree. The problem is that we never ask for only one exam. On one hand, patients love to do a full check-up “Please, test me for everything because my health plan will cover everything”. On the other hand, doctors love to ask for exams “I will ask for all the exams since blood will be drawn anyway”. In Brazil, doctors ask for an average of 1o to 20 tests per consulattion, depending on the specialization and health plan.
(OK, now it is time to PANIC) When we ak for 1 test, the chance of this test come back as NORMAL/NEGATIVE and the patient does NOT have the tested disease, is 95%, or 0.95. If we ask for 2 tests, the chances of both test come back normal and the patient does not have the tested disease is 0.95 x 0.95 = 0.9025. That means that there is about 10% of chance of one of the test come back as ABNORMAL/POSITIVE and the patient is healthy. If you consider 4 tests, the chances are 0.81 and when we achieve the number of 16 tests, the chances of one test coming back as abnormal is a THIRD!
The conclusion is quite important. Whenever I ask for a brazillion of tests, the chances that at least one of the results will come back abnormal and the patient is healthy is overwhelming. If I am, as I usually say, a doctor that is “hostage” of the exams, I will look for diseases where there are none! I will keep trying to fit the patient in the test results and not the opposite! This is what I call of “subsidiary patient, when the tests are what matter.
Some years ago, there was a trend in Brazil to take some flock of hairs and send them to USA, where they examined for almost all the elements in the periodic table! There were more than 50 exams. And who knows how the normal values for, let’s say, Cadmium, were established. The chance of at least one of the tests coming back as NOT NORMAL was close to 100%. Then, the doctor, in possession of the lab results, would say “Your Cadmium levels are high! We have to detoxify you!” and would prescribe you with some medicine. Some patients would become better, of course, and the rest of the herd would follow…
That’s something that is always on my mind: how many doctors today would have the guts to ignore a lab test just because it does not fit with the picture he drew from his patient? Hard question. Another: what kind of patients would believe his doctor if she/he decided to ignore the lab test? This one is easier: a patient that do not want to become subsidiary.
==================================
This post was written by Karl in his blog Ecce Medicus and translated by Carlos Hotta.

